

For the second entry in the clinical analogy series, we will be comparing how the pathophysiology of diabetes mellitus type II can be viewed as an analogy for cultural challenges in veterinary practices. Particularly, we will be viewing cultural challenges as a chronic disease that often presents in an acute-on-chronic state, and how a combination of predisposition (team composition, alignment with core values) and bad inputs/lifestyle (poor leadership) create the necessary environment for disease to occur.
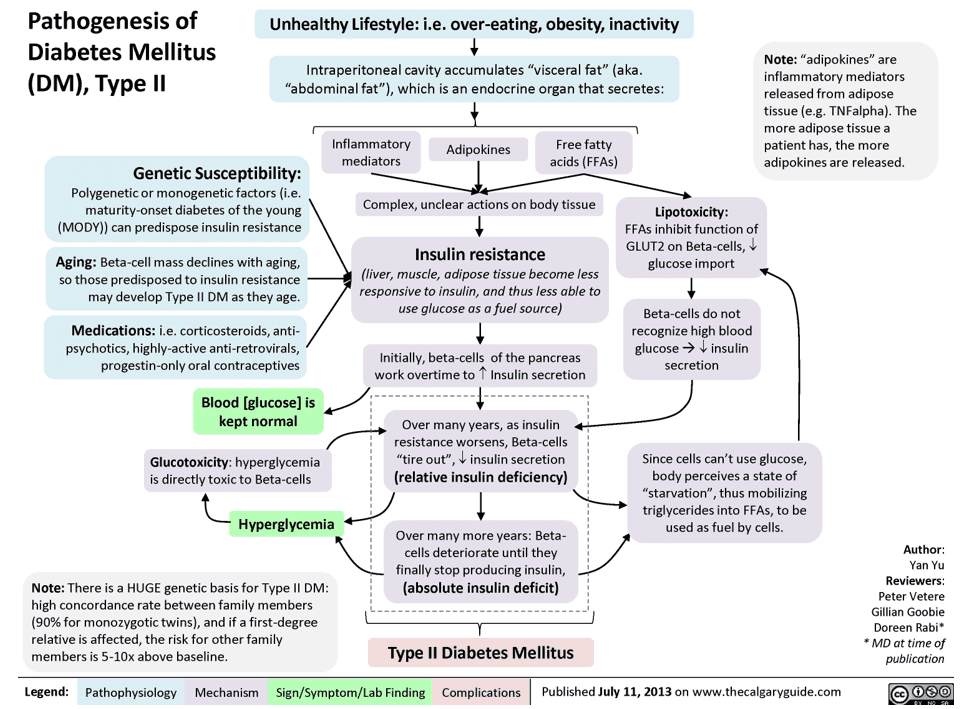
Diabetes Mellitus Type II is a complex metabolic condition that is hard to summarize without omitting or oversimplifying. In the spirit of not re-writing an entire textbook chapter, however, we can simplistically describe it as the combination of insulin resistance and insulin deficiency, leading to hyperglycemia and a variety of clinical sequelae.
Insulin resistance results from varying contributions from lifestyle and genetic factors. Insulin is a necessary mediator of the transport of glucose into cells, and when cells are less sensitive to insulin, they become starved of glucose even when sufficient glucose is available to them via the bloodstream. Inadequate glucose at the cellular level triggers signaling pathways that upregulate insulin secretion from pancreatic beta cells, creating compensatory hyperinsulinemia. For a time, the body can compensate for insulin resistance and blood glucose is normal. However, as insulin resistance worsens and beta cells become exhausted from chronic overproduction of insulin, insulin secretion drops and the compensated pre-diabetic state converts into Type II Diabetes where hyperglycemia and a cascade of other physiological derangements occur.
Source: https://calgaryguide.ucalgary.ca/pathogenesis-of-diabetes-mellitus-dm-type-ii/
Simplifying even further: Bad inputs (lifestyle) and predisposition (genetics) lead to improper function (insulin resistance). Compensation occurs for some time, masking the underlying disease (compensatory hyperinsulinemia), but eventually the compensatory mechanisms are exhausted, and overt clinical disease occurs (DM Type II).
Cultural challenges in veterinary practices follow a similar pattern:
Predisposition: Not having the right people in the right seats in the organization puts the clinic at heightened risk of cultural issues. To avoid this, a clinic needs to have a clear sense of what their core values are and have them front-and-center throughout all hiring and termination decisions.
Bad inputs: Even with the right people in the right seats at a practice, healthy culture requires ongoing inputs from clinic leadership. Negativity, lack of engagement, favoritism, and other negative inputs from leadership will drive poor culture. There needs to be a core set of competencies and expectations set for every role to ensure that team members have the right skills to succeed in those roles, know how success is defined and measured, and those standards must be uniformly applied to all relevant team members. Ambiguity is the enemy of confidence and fulfillment.
Culture crisis: An acute-on-chronic disease:
Sometimes, diabetic patients will arrive to the hospital in a state of acute-on-chronic illness such as diabetic ketoacidosis (DKA). In these circumstances, an undiagnosed or otherwise unregulated diabetic experiences some other insult to their health such as infection or other illness which triggers a much more serious metabolic derangement. As a result of a small additional push, these patients have rapidly decompensated from “not healthy, but getting by” to facing acute, life-threatening illness.
Clinics with underlying cultural concerns similarly sit in a fragile state, being one small push away from more severe manifestations such as open interpersonal conflict and/or mass turnover of team members. Importantly, it is not the small push that is the cause of this mismatched negative outcome, but rather the underlying cultural issues that have been brewing.
Addressing the crisis:
Just like DKA, acute culture crisis requires aggressive, immediate treatment.
Core values: Establishing a set of core values makes the process of determining what is broken with your team’s culture and how to fix it much simpler. Importantly, core values should be authentic to who the business is, not aspirational to what you think the business should be. Having a set of core values that is inauthentic or performative is worse than not having core values at all.
Look in the mirror as a leader: Addressing a culture crisis involves self-honesty around your own role in the problem. It is important to reflect on how are or aren’t you carrying the torch for your core values. For example, one of AVP’s core values is “Be Compassionate”. If I were to treat a team member at the AVP Success Center with unkindness, it would not only be an act inconsistent with those core values but also would signal to our team that those values will not be consistently applied throughout the organization, or perhaps are performative and won’t be applied at all. As leaders we are not exempt from aligning with core values, and if anything should conduct ourselves to the highest standards of those values. Nothing undermines buy-in faster than hypocrisy.
Assess your onboarding process: As you bring in new team members, the first 30, 60, 90, and 120 days needs to have a clear process that sets new hires up for success in terms of training, expectation setting, and culture building. Bad culture is highly contagious to hires if they don’t feel supported in their new roles.
Right person, right seat, aligned expectations: When a team is in a state of culture crisis, it is a moment to pause and assess whether you have the right people in the right seats within your organization, whether those people understand what is expected of them within their roles including a clear definition of what it means to succeed, and that they have the tools and training to achieve success. A culture crisis may result in the need to change personnel, but first you need to confirm that your team has been provided with the fundamental ingredients necessary to be successful in their roles and own the possibility that you’re dealing with a “you” problem rather than a “them” problem.
At Associated Veterinary Partners, we are proudly vet-founded, vet-operated, and not private equity controlled. If you are interested in learning more about how your practice could partner with AVP, please contact me at bilL@yourvetpartner.com. If you are interested in joining an AVP partner practice team, please go to the careers page at yourvetpartner.com to view open positions.
Your vet partner,
Dr. Bill Wagner